Gout: The Great Pretender | Heritage Hand & Plastic Surgery Okemos
This week, a patient returned to see me after I had previously removed an enormous gouty tophus from the back of one of his fingers, just at the middle knuckle. A tophus is essentially a tumor-like swelling of urate crystals; when they grow large, they can take on a distinct, lobulated appearance—almost cauliflower-like in texture.
He had been sent back to me by his occupational hand therapist because the area had suddenly become angry and red. How many times have I seen this? When I used to take emergency hand and face calls at Sparrow Hospital—which I did for 15 years—nearly every time I went on call, there would be one or two patients admitted for several days on intravenous antibiotics for a suspected infection. In reality, they likely weren’t infected at all, but were simply suffering from a flare-up of gout.
The “Demon” in the Joint
There are tremendous medieval accounts of gout, including famous illustrations depicting an evil devil biting into a patient’s foot. This describes the most common place gout affects people: the podagra, or the joint just behind the big toe.
However, as a surgeon, I frequently find gout in the wrist and hand joints, where it presents as though it is a serious infection. My patient today had his tophus removed surgically three weeks ago, but suddenly it was hot, red, and fluctuant—just like an abscess. In the office, I performed an aspiration of the fluid to ascertain whether this was truly an infection. Pessimistic, I was expecting to see a classic purulent abscess; instead, I found a bright white fluid that looks more like toothpaste than anything else.
On more than one occasion, I have been exploring a patient for tendonitis or synovitis (inflammation of the tendon lining), only to discover these bright, toothpaste-like white globules of deposits all around the tissue. That is when the penny drops: the patient has gout, and it hasn’t been treated medically.
The Anatomy of Filtration: A Family Connection
To understand gout, we have to understand how our bodies handle waste. Uric acid, as its name suggests, is largely excreted through the urine. It is a byproduct of the breakdown of purines, and in a healthy system, the kidneys act as a precision filter to keep these levels in check.
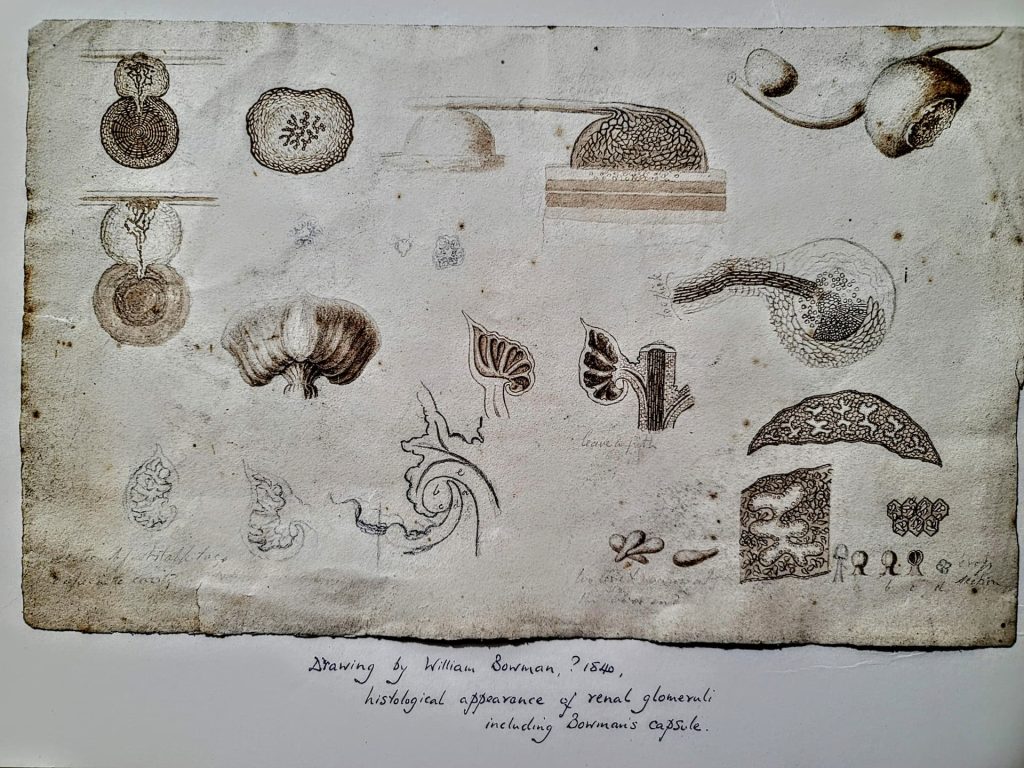
This process of filtration happens in a microscopic structure called the Bowman’s Capsule. This name has a special significance to me beyond my medical training. If you visit my waiting room, you will see my family history on display; my mother’s ancestors are direct descendants of the mid-19th-century surgeon Sir William Bowman.
Sir William was a pioneer in histology, and he was the first to realize that this capsule’s job is to separate small molecules—like water, salts, and uric acid—from the larger cells and proteins in the blood. We actually have his original sketches of the Bowman’s Capsule on display in our office. When this filtration system is overwhelmed or the kidneys aren’t clearing uric acid efficiently, levels in the blood rise. When the blood can no longer hold this excess, it “precipitates” out—much like sugar crashing out of over-saturated syrup—and forms those sharp, needle-like crystals in the joints.
Managing the “King of Diseases”
Historically, gout was known as the “Disease of Kings” because it was associated with the rich diets of the aristocracy. However, it could also be known as the “King of Diseases” due to how brutal the attacks are. A classic flare involves sudden, intense burning and a swollen, red joint so sensitive that even the touch of a bedsheet can be unbearable.
Dietary Advice for Reducing Risk:
The first line of treatment is reducing uric acid levels through dietary alterations:
- Limit High-Purine Foods: Avoid organ meats (liver, kidneys), red meats, and certain seafood like sardines or shellfish.
- Cut the Sugar: Reduce intake of high-fructose corn syrup and sugary sodas.
- Alcohol Moderation: Limit beer and grain liquors, which are high in purines.
- Hydrate: Drink plenty of water to help the kidneys flush out uric acid.
Medical Risk Factors:
- Obesity: Increases uric acid production.
- Kidney Disease: Impairs the ability to filter waste.
- Genetics: Your genes often dictate how your body processes purines.
- Hypertension & Diabetes: These conditions are frequently linked to gout.
If diet alone doesn’t work, medications like Allopurinol help reduce uric acid production. During a flare, high-dose non-steroidals (like Advil), Indomethacin, or Colchicine are used to stop the cycle. These are managed primarily by primary care physicians and rheumatologists.
The History of the Stout Tudor
King Henry VIII is the most famous historical sufferer. While it is often quoted that his physician said he suffered from a “surfeit of pears, port, and brandy,” this is the eye of the storyteller. Port hadn’t even been invented yet!
What he did have was the diet of an aristocrat: rich in red meat, game, organ meats, sweet wines, and fruit preserves. We know from depictions of the “Stout Tudor” that he became increasingly sedentary as he aged. While medieval doctors blamed “corrupt humors,” we now know those purine-rich feasts were the true culprit. Other famous sufferers include Charles V, Philip II of Spain, Benjamin Franklin, and even Isaac Newton.
Why is it the “Great Pretender”?
Gout mimics other diseases, most commonly infection. However, it can also look like:
- Other Arthritides: Rheumatoid, psoriatic, or regular osteoarthritis.
- Hand Conditions: It can masquerade as trigger finger, simple tendonitis, or carpal tunnel syndrome.
I recently released a man’s trigger finger only to discover that tell-tale “white toothpaste,” realizing he should have been treated with medicine and not my #15 blade. One frustration of diagnosing gout is that by the time symptoms peak, the uric acid in the blood has often “precipitated out” into the joint, meaning a blood test might return as normal. The body identifies these crystals as an “infection,” stimulating an inflammatory cascade that looks like major sepsis when no bacteria are present at all.
The Surgeon’s Role
Gout is not generally a surgical condition, but surgeons help identify it by taking biopsies and aspirations of joints. This assists primary care doctors and rheumatologists in correctly treating the right disease.
Next time you are in the office, feel free to take a look at Sir William Bowman’s original sketches in the waiting room—it’s a reminder that while our understanding of disease has evolved from “corrupt humors” to molecular filtration, the goal of the surgeon remains the same: finding the truth beneath the surface.





